 Robert Rover, MD a San Francisco Bay Area spine surgeon is performing a surgical technique to bring better outcomes in scoliosis surgery, as reported by Becker’s Spine Review.
Robert Rover, MD a San Francisco Bay Area spine surgeon is performing a surgical technique to bring better outcomes in scoliosis surgery, as reported by Becker’s Spine Review.
Dr. Robert Rovner: 3 Points on a New Technique for Better Outcomes in Scoliosis Surgery
Written by Laura Dyrda
Robert Rovner, MD, MBA, a spine surgeon, has developed a new technique for scoliosis correction. He discusses some ways in which the traditional surgery fails and how this new technique could create better outcomes in the future.
How current techniques can still fail patients
When a patient presents a case with severe scoliosis, surgery may be necessary to correct the problem. Early correction techniques involved fusions, but those procedures didn’t correct the curve; they only prevented it from worsening. Technology has evolved so surgeons can perform instrumentation for curve correction as well. Surgeons insert rods and attach them to the spine to bring the spine segments to the rods. For a more natural spine, surgeons can insert a curved rod. Some techniques involve rotating the rod 90 degrees so the scoliosis turns to a front-back curve. Once the rotation is accomplished, surgeons will then insert a second rod to strengthen the structure, bringing the spine to the second rod using screws, wires or hooks.
“In almost all available systems, two screws per bone are used up and down the curved portion of the spine and then a rod is attached to the screws on the left side. The second rod, on the right, is then attached to strengthen the construct, but all of the correction comes from the use of only the first rod, usually on the left,” says Dr. Rovner. “With the left rod in place, the second rod adds to the stability, but not to the correction.”
Scoliosis is both a curvature of the spine as well as a rotational deformity. This condition occurs when the ribs on the high side are rotated up as a result of the spinal rotation. Following traditional procedures, the end result can be disappointing for patients who are expecting to have the deformity corrected as well as the curve. As a result, Dr. Rovner wanted to find a way to improve these outcomes for his patients.
The solution: developing a new double-screw device
Dr. Rovner has developed a device that attaches the two screws together with a cross connector so surgeons have something to grip as they correct the deformity. “I can make the spine as straight as possible using the screws on both sides of the spine and then put in the rods,” he says.
The device, initially developed under Dr. Rovner’s guidance, is currently being fine-tuned by Synthes to make it more user-friendly. The procedure may be cumbersome for the moment, but Dr. Rovner anticipates that as he and other surgeons become more familiar with the technique, tweaks will be made to make the procedure easier and more efficient. “In the future, I think surgeons will start using this technique or something similar because of the proven benefits for their patients,” he says.
What it takes to train on the procedure
Scoliosis surgery is a difficult procedure which often necessitates extensive fellowship training to perform with good outcomes. But in using the traditional techniques, even the best surgeons can have an imperfect outcome, which Dr. Rovner says is frustrating. Using this new device and technique, however, could help improve these outcomes.
“The technique and device may be a bit more challenging, but as the results improve, we’ll start to see more surgeons use it in the future,” he says. “There are some surgeons who learn one technique and never change, but most surgeons constantly update their techniques as new technology becomes available.”
For those who are interested in learning more, surgeons can look at a technique manual or watch someone do a few of these operations to become familiar with the device and adverse issues that can occur. In the end, other surgeons should be able to pick up the procedure fairly easily — the instrumentation is different, but the screws and rods are the same.
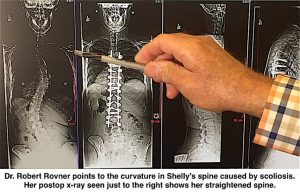 Scoliosis is an abnormal, often progressive curvature of the spine that also causes the spine to rotate. Danville, CA spine surgeon Robert Rovner, MD has developed a new technique and surgical hardware to more fully correct the spine’s rotation for the first time. This rotation can create a telltale “rib hump” which is not fully corrected by conventional surgical procedures. “I believe this procedure can provide the best outcomes compared to the currently available treatments for scoliosis,” says Dr. Rovner.
Scoliosis is an abnormal, often progressive curvature of the spine that also causes the spine to rotate. Danville, CA spine surgeon Robert Rovner, MD has developed a new technique and surgical hardware to more fully correct the spine’s rotation for the first time. This rotation can create a telltale “rib hump” which is not fully corrected by conventional surgical procedures. “I believe this procedure can provide the best outcomes compared to the currently available treatments for scoliosis,” says Dr. Rovner.