Cervical Disc Replacement
In the neck, the discs between the vertebral bodies can herniate or bulge and push on the nervous system directly behind it.
The nerves in the neck include the spinal cord and the nerve roots. There are II nerve roots that leave the spine at each level (a left and a right). Each of these nerves are responsible for stripe of skin radiating into the arm and a specific muscle. Also this type of nerve irritation can keep pain on the inside border of the shoulder blade.
The C4 nerve root (C means cervical) controls the deltoid and its numbness travels from the neck to the shoulder pad and just into the upper arm.

The C5 nerve root controls the biceps and the deltoid and its numbness travels to the thumb side of the forearm.
The C6 nerve root controls the biceps and wrist extension and its numbness travels to the thumb index and the middle fingers.
The C7 nerve root controls the biceps and wrist flexion and is numbness travels to the ring and little finger.
The C8 nerve root lies between the C7 and T1 vertebral bodies (the T1 vertebral bodies the top bone of the thoracic spine). The C8 nerve root controls the finger spreading apart and the wrist moving towards the little finger. The C8 numbness travels to the little finger.
Cervical disc replacements are not for every patient. Patients that have excessive arthritis in the side joints of the disc (UV joints, Luschka's joint) are not the best candidate for this type of technology. Patients that have a minimal amount of arthritis in these joints and a bad disc that is pushing on a nerve root or the spinal cord are better candidates for disc replacements. Furthermore there are backside joints of the neck called facet joints and if those facet joints have a fair amount of arthritis then it is likely better that the patient gets a fusion at that one particular region.
The benefit of the cervical disc replacement is to provide stability and support between the 2 bones and allow for normal motion in the region of the cervical spine. This is thought to preserve the discs above and below the operation. Oftentimes when we fuse patient's to see degeneration above or below the level of the fusion within about 10 to 15 years.
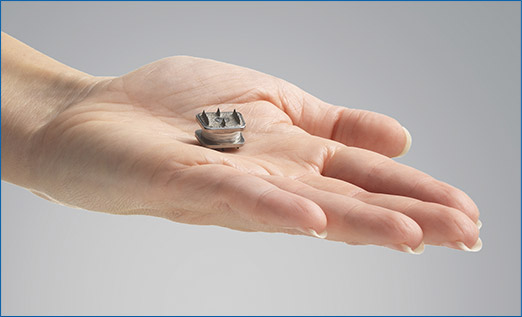
The newest disc to come out in America is the M6 disc from Orthofix (SEE FACT SHEET). It has been used in Europe for the last 12 to 15 years and has a good track record of safety and effectiveness. I have been implanting these discs and my patients over the course the last 2 years. My patients are doing well and I have not observed any complications using these devices in my patients’ operations. In fact it is allowed several patients to get back into their difficult jobs including nursing and law enforcement.
The operation to place a cervical replacement disc occurs through the front part of the neck. The approach is between the muscle and the swallowing tube and the breathing tube. Usually patients do very well after the surgeries and they do not suffer any major ill effects. Occasionally patients will have swallowing issues after this operation because the esophagus has to be gently mobilized away from the front part of the spine to do this type of operation. That can cause a week or 2 of difficulty swallowing. Only rarely does a cause ongoing swallowing disorders. Because the approach also retracts the breathing tube the operation can irritate the nerve that goes to the vocal cord. This effect is usually transient and rarely patients can have voice changes long after surgery. Infections, nerve injuries, bleeding can happen but these complications are very rare.
The positive effects of the surgeries can be striking. Once I had a patient that had a pain for 25 years in the same arm. And in one day, all of her pain was gone. The patient was ecstatic. She could now use her right arm normally.
The cervical disc replacement operation is easy to perform and, from the patient's perspective, relatively easy to go through.